Epidemiology Corner: Tuberculosis
For as long as human civilization has existed it has had a companion: Tuberculosis. Known historically as consumption, the White Plague, and phthisis; it has periodically reared its head throughout history to claim millions of lives. It is perhaps the deadliest pathogen in human history and even now presents as a threat to world health.
This disease is caused by a bacterium called Mycobacterium tuberculosis, which infects the lungs and is transmitted through coughed up droplets. Tuberculosis can remain dormant for years the remerging to cause a devastating illness. Symptoms present as coughing, chest pain and fevers. If untreated the disease will persist for years, it is always devastating and often leads to death.
Fortunately Tuberculosis can be stopped with antibiotics and is no longer as fatal. But the disease can hide in the lungs dormant for years. In places without access to healthcare is just as deadly.
The Culprit:
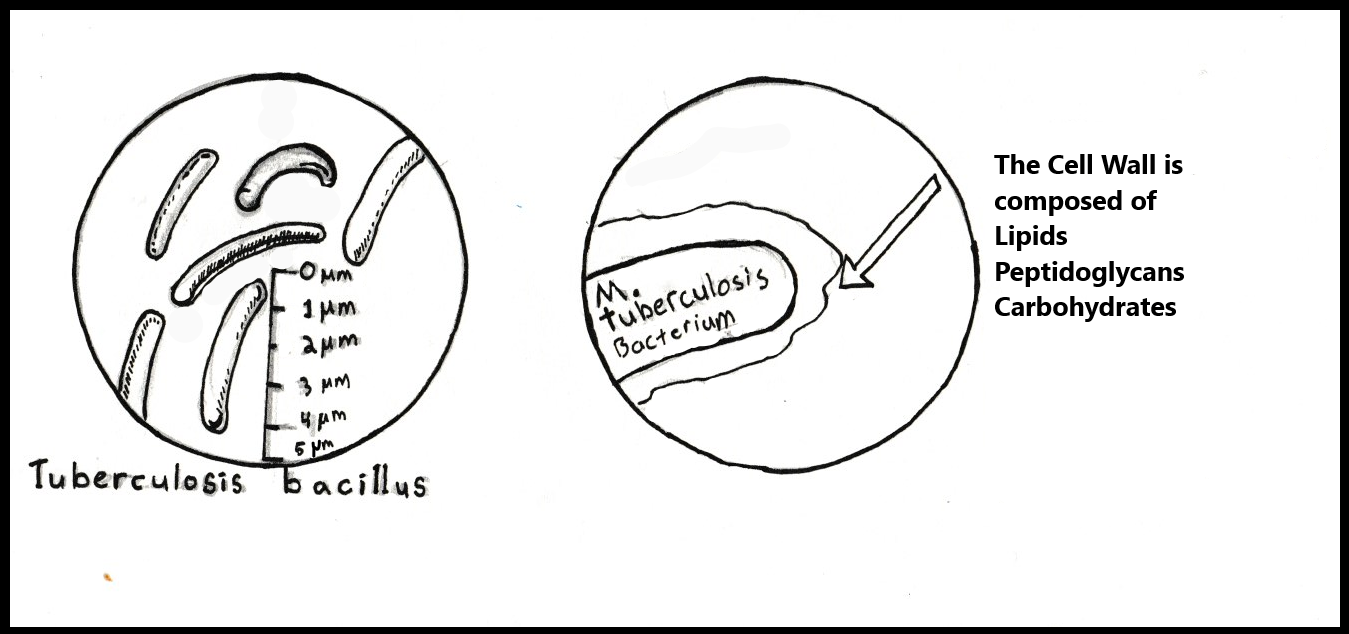
M. Tuberculosis is a rod-shaped bacterium. It is 2-4 micrometers (uM) and 0.2-0.5 uM in width. This is much smaller than the cells of the human body. A macrophage, the cell type M. tuberculosis initially infects, is typically 21 uM across. The bacterium requires oxygen to replicate and cannot move on its own. It is well suited to the environment of the human lungs which provide oxygen and can cough and expel the bacteria into the air. M. Tuberculosis is notable among bacteria for two reasons: it’s incredibly resilient cell wall and its lengthy division. Bacteria, like eukaryotes (you, me, the bees, the trees) have a plasma membrane composed of a phospholipid bilayer. This is the membrane that contains the cell and all its components. Some bacteria create another wall outside of the phospholipid bilayer called the cell wall. M. Tuberculosis possesses an elaborate and unique cell wall. It is, like most bacterial cell walls, made up of fats, proteins, and sugars. The wall is mostly composed of complex lipids (fats), but it also has peptidoglycan (sugars connected to proteins) and polysaccharides (complex carbohydrates) that dictate the structure and viability of the cell. The cell wall and the structures on it are how the bacteria interacts with the world around it. The second notable aspect of M. Tuberculosis is that it takes 12-20 hours to replicate. This is ten times longer than most other bacteria; E. coli can replicate once every twenty minutes. This seemingly simple aspect provides another defense against treatment by shortening the window in which antibiotics can attack.
M. Tuberculosis spreads through droplets and sputum coughed up or exhaled by an infected person, the same mechanism coronaviruses and the flu use transmit disease. Once inhaled by a new host these disease carrying droplets travel to the lungs. The presence of foreign cells triggers an immune response and cells called macrophages respond. Macrophages are a type of white blood cell that engulfs foreign material such as debris, bacteria, viruses, and cancer cells. The process of engulfing is called phagocytosis. It starts when the macrophage engulfs the target. The enclosed particle buds off inside the cell in a small bubble of membrane. Once inside the macrophage the bubble of cell membrane is called a phagosome, which matures into a lysosome. The inside of a lysosome is very different from the rest of the cell, it is highly acidic and contains enzymes for breaking down cellular structures.
M. tuberculosis acts like a Trojan Horse, it offers itself to the macrophage to be eaten up. Once inside the macrophage M. tuberculosis halts the maturation of the phagosome into a lysosome. Now that it is within the cell the bacteria begins to reproduce safe from attacks from the immune system. Many bacteria use a similar system of avoiding destruction by macrophages such as Listeria, Shigella, Legionella, and Salmonella, all of which cause serious disease.

At this point in the infection there are two ways the disease can progress. Latent or dormant Tuberculosis arises when infected macrophages emit chemicals known as chemokines to attract other immune cells. These immune cells are not effective at disposing of the bacteria. But the accumulation leads to the formation of lesions composed of more immune cells. Inside this ball of cells the bacteria cannot spread, there is no oxygen and it is too acidic. Once the host develops immunity the disease carrying macrophages are destroyed. This process forms hard solid masses inside the lung indicative of a tuberculosis infection. Not all of the bacteria is destroyed though, and small amounts of M. tuberculosis lay dormant in the lungs waiting for an opportunity. In this stage tuberculosis is not contagious, merely waiting.
Once the immune system of the host becomes compromised, whether through disease, injury, or age, the bacteria emerges and renews its attack. This phase of the disease, lasting around 3 months but sometimes for years, is active Tuberculosis and if left untreated is as fatal as often it isn’t.
The bacteria may travel to other organs and will disseminate throughout the lungs. The membranes surrounding the lungs can become inflamed, causing enduring chest pain. The infection will cause persistent fever, chills, and fatigue. Decreased appetite and subsequent weight loss are common. Coughing up of sputum and blood is the calling card of tuberculosis. The disease is now very contagious and easily spreads through contact and inhalation of aerosol droplets. Tuberculosis is particularly prevalent in HIV positive population causing severe and dangerous infections for those with compromised immune systems.
Treatment:
Luckily Tuberculosis is a treatable disease. Modern antibiotics allow us to reverse the once certain death sentence. A number of antibiotics are used against the bacteria all attacking different aspects of its biology. There is also a good deal of secondary treatment for tuberculosis as well as palliative care.
The four antibiotics recommended by the CDC are isoniazid, ethambutol, pyrazhamide, and rifampin. The first three all interrupt the process of cell wall synthesis. As mentioned earlier, the cell wall is a vital component to the viability of M. tuberculosis. Unfortunately these antibiotics are biostatic, meaning they only work when the cell is dividing. This is why tuberculosis treatment can take 6-9 months. The bacteria are most vulnerable when dividing, which they do very slowly, and can often lay dormant.
Rifampin specifically attacks the synthesis of RNA in the bacteria. Unlike the others it will interrupt the normal activity of non-dividing M. Tuberculosis cells. However Bacteria will develop resistance to any one of these antibiotics, but their use in tandem is often enough to destroy the invader.
Unfortunately M. Tuberculosis, like many other bacteria, is excellent at adapting to new threats and has the potential to become antibiotic resistant. An AB-resistant strain will likely only be protected from one or a few antibiotics, but it presents a critical situation that requires very specific treatment. People with a compromised immune system, such as cancer patients and the HIV-positive, are particularly susceptible to M. Tuberculosis. The method of treating tuberculosis in the immunocompromised and antibiotic resistant strains involves a very intensive mixture of the same drugs and rigorous observation.
History:

Genetic analysis suggests that M. tuberculosis might be 15,000 years old, but this is not conclusive. Other research suggests a more recent date, 6,000 years ago. Paleopathological (the study of disease in ancient remains and fossils) evidence shows lesions associated with tuberculosis on the bones of Egyptian mummies dating back to 3700 BC. However the Ancient Egyptians did not record the existence of the disease. The first written description of Tuberculosis is in an ancient Indian text from around 1300 BC, and another notable record from China around 300 BC. Referred to as phthisis by the ancient Greeks, Hippocrates describes tuberculosis in quite accurate detail. We know that M. tuberculosis was present in the Americas as well because of lesions on the bones of Peruvian mummies dating from well before European contact.
Throughout ancient and Medieval history tuberculosis remained a constant and deadly presence within world populations. The scientific and industrial revolutions brought new understanding of the disease, but it spread quickly in densely populated cities. The eighteenth century marked the beginning of modern tuberculosis pandemics. Hundreds of thousands were dying every year, young and old alike.
By the nineteenth century the development of particularly poor living standards in cities of European countries made perfect conditions for the spread of tuberculosis. The disease was ubiquitous across Europe and North America. The symptoms were so common they even became romanticized in nineteenth century European culture. The pale skin and swooning nature of consumption, as it was called, appealed to the sensibilities of the time period.
The current fear regarding Covid-19 is a good comparison for the historical terror of tuberculosis. It was not completely understood, many could carry the disease and not know it, and it could bring on an agonizing illness. Luckily Tuberculosis, unlike Covid 19, cannot be passed along by someone who doesn’t show symptoms. But that fact, and other realities we would consider common sense, would have been unknown. In the nineteenth century tuberculosis was a fixture of history that was lethal, uncurable, and constant.

That all changed as scientist and doctors using the framework of the scientific process to learn about the disease. Prussian doctor Robert Koch pulled back the mask to reveal the true face of tuberculosis in 1882. At that time scientists were just beginning to properly isolate, culture, and identify bacteria. Using a serum of blood, Dr. Koch incubated M. Tuberculosis. He then took this isolated bacteria and infected rabbits with it. The rabbits displayed symptoms of tuberculosis and proved the M. Tuberculosis was the causative agent of tuberculosis.
Though the barrier of identifying the cause of the disease had been overcome it was still largely untreatable. Specific institutions began opening to attempt treatment and provide care for tuberculosis patients. These sanitaria opened up all across America and Europe. They treated the disease by providing an environment with “clean air”; the convention of the time stipulated time away from the harsh city environment would help patients’ bodies to heal. A refreshing vacation away from the unsanitary conditions of 19th century city life could have been of great benefit to the immune system. This could have been efficacious. Tuberculosis Is an opportunistic disease and by leaving the harsh city environments it might have given patients’ immune systems a chance.

In 1943 when a PhD student named Albert Schatz, along with other members of a Rutgers’ Lab Elizabeth Bugie, and Selman Waksman, isolated a compound produced by Streptomyces griseus. The chemical was called streptomycin, it was produced by S. griseus to fight other bacteria, and it was an effective antibiotic against many disease-causing bacteria. By 1946 streptomycin had been used successfully to cure patients of Tuberculosis infections. In 1952 an antibiotic called isoniazid was developed that could be taken orally to safely stop and cure tuberculosis infections. Finally the grim specter of consumption was beaten back by the concerted efforts of scientists across nations and centuries.
The Future:
Despite tuberculosis being a manageable disease in developed nations it still remains endemic and destructive. As has happened with many once treatable bacteria, M. Tuberculosis is developing resistance to even the most potent antibiotics. The cost of treating drug resistant bacteria, in both lives and resources, is increasing each year. One can’t help but predict cities once again held hostage by a pandemic of incurable antibiotic superbugs, given the 500,000 cases of multidrug resistant tuberculosis arising each year according to the WHO.
In developing nations, the battle with tuberculosis still rages. According to the WHO, southeast Asia accounts for 41% of global cases. It’s easier to forget the cost of life in other countries than we care to admit. Even though humanitarian concern should be enough for us to try and drive tuberculosis extinct it often isn’t. Some studies indicate that up to 30% of the population have either latent or active tuberculosis. But as this recent pandemic shows, respiratory diseases afflicting one nation can soon strike populations on the other side of the globe.
As sensational and clickbait happy as it would be to decry all hope the scientific and medical communities are pushing the fight against Tuberculosis. The WHO, CDC, Gates-foundation, and a bevy of other organizations are working tirelessly to rid humanity of one of its oldest tormentors. Like many other healthcare concerns the Covid Pandemic has put these causes on the back burner. Hopefully, we will soon resume the proud task of curing humanity of Tuberculosis.
Addendum:
Tuberculosis is not always fatal, but still is very often lethal. Credit: u/thecave from reddit.
References:
Daniels, T.M., 2006, The History of Tuberculosis. Respiratory Medicine Vol. 100 Issue 11.
Barberis, I., Bragazzi, N.L., Galluzzo, L., Martini, M., 2017, The History of Tuberculosis: from the First Historical Records to the Isolation of Koch's Bacillus. Journal of Preventative Medicine and Hygiene. E9-E12
Kapur, V., Whittam, T. S., Musser, J. M. ,1994. Is Mycobacterium Tuberculosis 15,000 Years Old? Journal of Infectious Diseases.
Brosch, R., et al, 2002, A New Evolutionary Scenario for the Mycobacterium Tuberculosis Complex. Proceeding of the NAtional Academy of Science of the United States of America.
Nguyen, L. ,2016, Antibiotic Resistance Mechanisms in M. tuberculosis: an Update. Archives of Toxicology.
Alderwick, L. J., Harrison, J., Lloyd, G. S., & Birch, H. L. ,2015, The Mycobacterial Cell Wall—Peptidoglycan and Arabinogalactan. Cold Spring Harbor Perspectives in Medicine.
E. L., Watt, C. J., Walker, N., Maher, D., Williams, B. G., Raviglione, M. C., Dye, C. ,2003, The Growing Burden of Tuberculosis. Archives of Internal Medicine, Harbor Perspectives in Medicine.
WHO staff, 2020, Tuberculosis. Retrieved from https://www.who.int/news-room/fact-sheets/detail/tuberculosis
CDC staff, 2020, Tuberculosis. Retrieved from https://www.cdc.gov/tb/default.htm
CDC staff, 2020, Treatment for TB Disease. Retrieved from https://www.cdc.gov/tb/topic/treatment/tbdisease.htm
Zimmer, C., 2014, Tuberculosis Is Newer Than Thought, Study Says. New York Times, Retrieved from https://www.nytimes.com/2014/08/21/science/tuberculosis-is-newer-than-what-was-thought-study-says.html?_r=0